Lesson 3: Ischemia
- Tooba Alwani
- Feb 27
- 2 min read
Updated: Mar 27
Summary of Learning Points
Definitions myocardial injury vs ischemia vs infarct
Injury - troponin rise due to some insult (+/- ischemia)
E.g STEMI (ischemic), myocarditis (nonischemic)
Ischemia - insufficient O2 to myocardium (+/- infarct; +/-injury)
Symptoms (e.g. Chest discomfort), new ECG changes, new wall motion abnls, or new thrombus
E.g. STEMI (infarct+injury), stable angina (no infarct, no injury)
Infarct
Myocardial necrosis from ischemia
E.g. STEMI, NSTEMI
ECG accuracy can vary immensely depending on numerous factors (reader experience, lead placement, timing of ischemia, underlying arrhythmias, artifact)
ECGs evolve in ongoing ischemia
Always compare to baseline ECG, and trend ECGs if in doubt
Pathologic Q waves are deep and/or wide
>1mm deep or 25% of QRS
>40ms wide
Can be seen in NEW or OLD infarct
ST Elevations
>0.1mm in 2 contiguous leads (V2 and V3 threshold higher >0.2mm)
exception: STE in avR = BAD (usually 3 vessel disease or L main disease)
If you see other ischemic signs like pathologic Q waves, St depressions, TWIs, always look closely for ST elevations
Consider posterior infarcts! (get V7-V9 leads, or right sided leads)
Localize to coronary distribution (assuming typical anatomy) unlike ST depressions which do NOT localize
Usually due to transmural infarct
ST elevation morphology
Concave (smiley face) = usually not MI e.g. pericarditis
Convex (frown) = usually MI
Other causes of STE: pericarditis, LBBB (use Sgarbossa's to help dx MI), LVH, strain, Brugada, early repol, aneurysm, PE)
ST Depressions
New horizontal or downsloping depression >0.05mV in 2 or more contiguous leads
Does not localize to coronary territory!
Suggests subendocardial ischemia
T Waves
Positive deflection (ventricular repolarization) after QRS
EXCEPT: avR, V1, III
Hyperacute T waves: TALL, broad, asymmetrically peaked
Ominous sign as it can be first sign in evolving STEMI
T Wave inversions
>0.1mV in 2 contiguous leads
Do NOT localize
Can be sign of ischemia
can also be seen in non-schemic conditions (strain patterns, PE, myo/pericarditis, cerebral T waves)
Wellens Syndrome
T wave abnormality occurring during CP-free time c/f CRITICAL L coronary disease
Type A = biphasic in V2-V3 (up then down)
Type B = deep inverted T waves in precordium
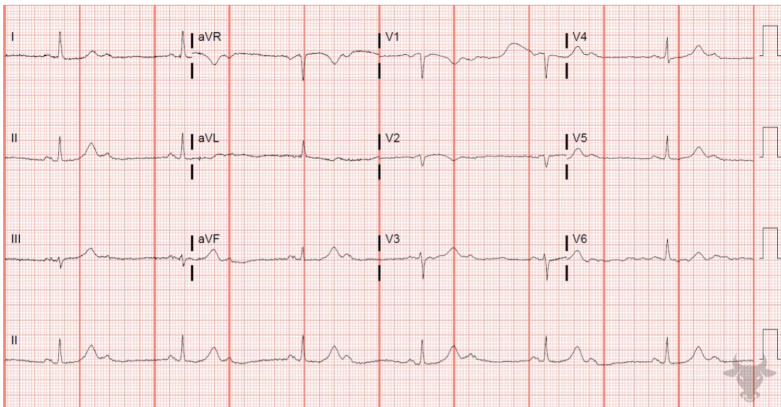
Practice ECG
Answer