Lesson 2: LVH/RVH and Strain
- Tooba Alwani
- Feb 27
- 2 min read
Updated: Mar 27
Summary Of Learning Points
LVH increases the amplitude of the normal vector generated by the left ventricle.
This results in a deeper S wave in earlier septal leads and a taller R wave in later septal leads and lateral leads
There are many criteria for LVH (you don’t need to memorize these!), some of the most common include
Cornell Criteria: S wave in V3 + R wave aVL >28mm in males >20mm in females
Sokolow-Lyon Criteria: S in V1 or V2+ R in V5 or V6 >35mm
Any precordial lead is ≥ 45 mm
The R wave in aVL is ≥ 11 mm
The R wave in lead I is ≥ 12 mm
The R wave in lead aVF is ≥ 20 mm
LVH with strain is characterized by
ST depression with downward concavity and asymmetric T wave inversions in V4-V6
ST elevation with upward concavity and upright, asymmetric T wave in V1-V3
With abnormal depolarization there is often abnormal discordant repolarization.
RVH increases amplitude of the normal vector generated by the Right ventricles
This manifests as an R:S ratio >1 in leads V1 and V2
RVH criteria: R:S ratio >1 in leads V1 and V2 AND 1 of the following
Right atrial enlargement
Right axis deviation
RVH strain
S1Q3T3
RVH is a challenging diagnosis! R:S >1 alone is not diagnostic of RVH, differential includes
Right ventricular hypertrophy
Right bundle branch block
Posterior wall AMI
WPW type A
Young kids and adolescents
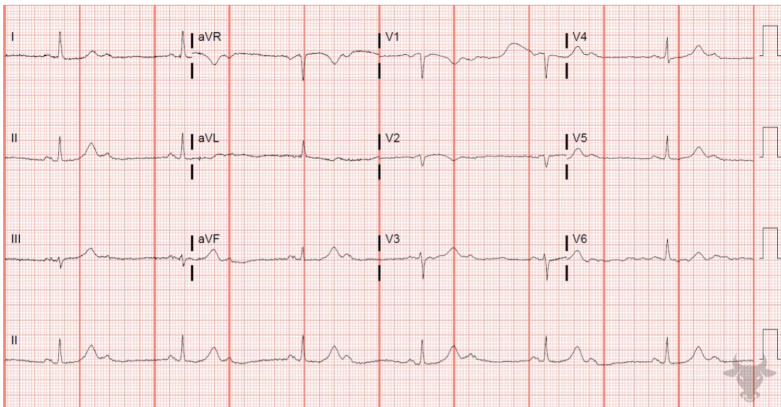
Practice ECG
Answer