Lesson 6: Bradycardia
- Tooba Alwani
- Feb 27
- 2 min read
Updated: Mar 27
Summary of Learning Points
Cardiac Conduction:
Sinoatrial (SA) node atrioventricular (AV) node bundle of HIS and left/right bundle branches ventricles
PR interval:
Time it takes depolarization to spread from the SA node to ventricle
Normal PR interval < 200 ms or less than 5 small boxes on EKG
Bradycardia: Heart rate < 60
Sinus Bradycardia:
Sinus rhythm with heart rate < 60 due to decreased sinus node activity
Meds*, Vagal tone, Hypothyroidism, Anorexia, Hypothermia, Myocarditis
First Degree AV delay:
PR interval > 200 ms due to conduction delay from SA node to ventricles
Meds*, Vagal tone, age related disease, infiltrative disease
Second Degree Heart Block: intermittent conduction of atrial activity to ventricles
Mobitz I (Wenckebach):
Progressive lengthening of PR interval prior to non-conducted p wave due to AV node fatiguability
Meds*, vagal tone, inferior MI, myocarditis
Mobitz II:
Intermittent non-conducted p waves without progressive prolongation of the PR interval due to structural conduction failure below AV node
Meds*, anterior MI, idiopathic fibrosis, inflammatory conditions (rheumatic fever), autoimmune (SLE), infiltrative (amyloid, sarcoid)
Fixed Ratio
2:1 Block
Every other p wave is dropped so cannot distinguish between Mobitz I and II
Increase sympathetic drive (exercise) - block improves Mobitz I
Increase vagal tone - block improves Mobitz II
High Degree: 2 or more non-conducted p waves
Complete Heart Block:
No association between p waves and QRS. Wide complex.
Supraventricular impulses not conducted to the ventricle. The ventricle is excited by an escape mechanism (junction or ventricular).
AV node fatigue (acute phase of an inferior MI), conduction failure, meds*
Treatment of Unstable Bradycardia with a pulse - atropine, epinephrine infusion, dopamine infusion, transcutaneous pacing
*beta blockers, calcium channel blockers, digoxin, amiodarone, opiates
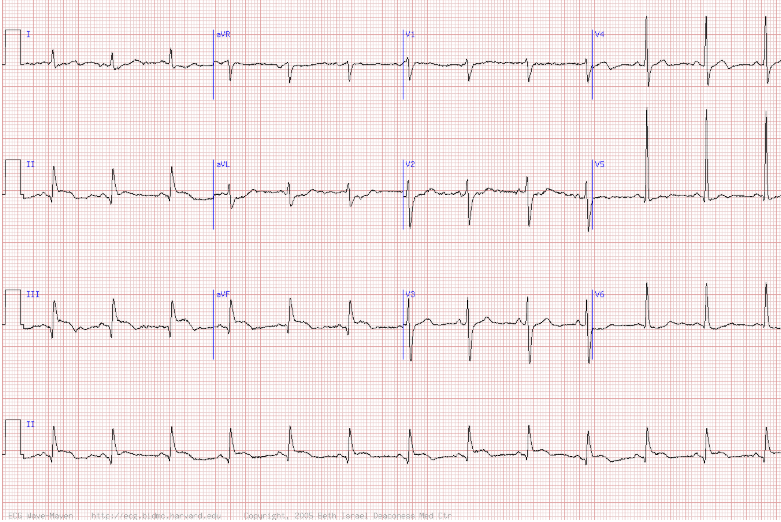
Practice ECG
Answer